Botox for cervical dystonia
There are links throughout this FAQ to medical journals and scientific research if you want to learn more about the recommendations here.
- Botox for cervical dystonia
- 1. How can I find a doctor to do my botulinum toxin injections?
- 2. What should I look for in picking a doctor to do my injections?
- 3. What is “EMG” I keep seeing people talk about?
- 4. Can only neurologists do injections?
- 5. How exactly will botox injections help me?
- 6. How many rounds will I need?
- 7. How should I prepare for the injections?
- 8. What sort of post-injection aftercare should I do?
- 9. How long do the shots take to work?
- 10. How long do the injections last?
- 11. Are there side effects from the injections?
- 12. Which muscles should I get injected?
- 13. Can botox reduce or eliminate tremors?
- 14. Should I do physical therapy if I’m getting injections?
- 15. What should I do if the injections aren’t helping me?
- 16. Is it really worth it to try switching doctors if botox hasn’t worked? Why would that help?
- 17. What should I do if the injections stopped working?
- 18. I heard botox only helps a small percentage of CD patients – is that true?
- 19. Can I get injections more often than every 3 months?
- 20. What are the differences between the various botulinum toxin brands?
- 21. Are there long-term concerns about getting botox injections?
- 22. How do I pay for injections?
1. How can I find a doctor to do my botulinum toxin injections?
If you’re in the U.S., use the Dystonia Medical Research Foundation’s doctor directory search to find a movement disorder neurologist who treats cervical dystonia: https://dystonia-foundation.org/directory/categories/find-a-doctor
If you’re in the UK, find doctors who administer botox injections for dystonia here: https://www.neurotoxinnetwork.org/uk-botulinum-toxin-service-map/
If you’re in Canada, find providers here: https://dystoniacanada.org/support
If you’re in Australia, look here: https://dystonia.org.au/living-with-dystonia/movement-disorder-neurologists/
If you’re in Europe, you can find dystonia treatment centers here: https://www.ern-rnd.eu/disease-knowledge-hub/dystonia/ern-rnd-centres-dystonias-paroxysmal-disorders-nbia/
2. What should I look for in picking a doctor to do my injections?
First, the doctor should have experience in cervical dystonia (CD). Usually, that means a neurologist who specifically specializes in movement disorders. That also usually means you should not see a general neurologist for injections. You need someone with expertise in CD.
Multiple studies show that the single most important factor in the success or failure of botox injections is the doctor who does it. When people don’t respond, it’s usually because their doctor is not injecting the correct muscles or using the correct doses. CD is different in everyone so there is trial and error in figuring out the right combination of muscles and dosing, but if you’re not seeing any results after three or four rounds, it could be worth looking for another doctor.
Second, at a minimum your doctor should use EMG. (Explained in the next question.)
Another factor that could help, especially if you have a more challenging case of CD that requires injecting deep muscles, is the use of ultrasound. Ultrasound is when the doctor puts goo on your skin and rubs a wand over your skin to see the muscles underneath using sound waves. With ultrasound, a doctor can better visualize the muscles and be more precise with injections. It also also allow doctors to be more consistent with their injection placement from round to round. While EMG has become relatively common and should be expected, many doctors don’t use ultrasound (even though they really should. Some neurologists use it, but you may find more PM&R doctors (physiatrists) use it.
(If you have a disorder that causes hypermobility, like certain types of Ehlers Danlos, make sure your doctor knows before doing any botox as it can cause head instability in people with hypermobility. You may want to seek out a doctor who has experience treating CD in people with hypermobility.)
Bottom line: It’s important to understand that CD is not the sort of condition where you can see just any doctor. The treatment is not a pill that any doctor can prescribe you. And it’s not an injection that is in the same spot for everyone that any doctor can do. Every patient requires a unique injections tailored to them, which means you need a doctor with the knowledge, skill and willingness to work with you to figure out the best injections for you.
3. What is “EMG” I keep seeing people talk about?
It is highly recommended you see a doctor who does EMG-guided injections. EMG is short for electromyography. In EMG injections, a wire is attached to the injection needle that will measure your muscle activity. It’s connected to a machine that represents muscle activity by static sounds. When relaxed, muscles should be quiet. When they are dystonic and overactive, even when you’re relaxed, they will make loud crunching sounds. That tells the doctor to inject that muscle.
Studies show using EMG leads to better outcomes and ensures doctors aren’t injecting non-dystonic muscles or missing muscles that are dystonic. If your doctor is not using EMG, there’s no way they can be sure if a muscle of yours is dystonic or not, especially a muscle that cannot not be palpated (felt by hand), which many neck muscles cannot because they overlap each other.
Here is an example of what EMG-guided botox injections are like in this video:
Another less common use of EMG is EMG mapping. In EMG mapping, the doctor isn’t injecting you with botox – instead, your doctor will insert the EMG needle into all the muscles in your neck to “map” which are dystonic and which aren’t.
Not all doctors offer EMG mapping since your doctor should be able to identify possible dystonic muscles based on the pattern of how your head turns, but studies do show it can improve outcomes for patients. Your doctor may not offer unless you ask, so it can be worth asking before your first set of injections.
4. Can only neurologists do injections?
No, while many people do get their injections done by neurologists specializing in movement disorders, some people have found success by seeing a physiatrist (also known as a PM&R, or Physical Medicine and Rehabilitation doctor) or a pain management specialist. Your insurance company may require that the doctor you see for injections falls into those three categories.
If the doctor has a lot of experience doing cervical dystonia injections and uses EMG, they may be a good option, even if they aren’t a neurologist. Experience and familiarity with CD is key.
5. How exactly will botox injections help me?
When the right muscles are targeted with the right amount, you should expect a reduction in the pulling feeling and abnormal head position, reduced pain and/or reduced tremor. (Not everyone has pain. Somewhere around half of people don’t have tremor. And not even everyone has abnormal head position. So it depends on what you are trying to address.)
It likely won’t make all your symptoms disappear 100%, but good results can significantly reduce symptoms and make remaining symptoms more minimal and manageable. It’s important to have the right expectations: you should not expect injections to make all your symptoms completely disappear, but you should expect and work with your doctor toward noticeable and meaningful improvement. If your injections are helping, but you’re only getting, say, 20% improvement, that’s not enough and you should either work with your doctor to improve the dosage and placement or switch to another doctor.
Injections are unlikely to hit their maximum benefit the first time, and sometimes the first round doesn’t help at all – this is normal, so don’t worry. Usually the doctors start with a lower dose than they think you need, and then slowly work up from there in subsequent appointments. The doctor will also probably start with obvious muscles to inject first, before slowly adding others or trying different muscles based on how you respond. This is done to avoid side effects and to evaluate what’s helping or not.
In other words, you need to have patience as it can take a few rounds, but ideally each round will get incrementally better and better. The benefit from injections is a marathon, not a sprint. One study found optimal results took at least four visits (which takes one year), but some sub-types took more. Take good notes in between botox rounds and give your doctor clear and specific feedback so your doses and injection sites can be fine-tuned for your next round.
According to research, people who have had CD for a long time without treatment respond worse to injections than people who start shortly after onset, and so injections should be initiated as soon as possible.
This study found that after three years of getting injections, baseline head position had improved, so there may be a cumulative effect of injections over time.
One study found that botox injections improve anxiety in people with CD, independent of the improvements botox has on the dystonia.
One study found that botox restored normal sensorimotor network activity in the brains of people in CD.
Anecdotally, many older people who have been on botox for years report it has allowed them to live a completely normal life: they worked full-time jobs, got married, had children, etc.
6. How many rounds will I need?
The injections last around three months, and you will need to keep getting injections every three months as long as you continue to have symptoms. Unless you go into remission or you are able control your symptoms another way, this means you might continue getting the injections indefinitely.
Some people are fortunate enough that they start seeing significant results on their first round of injections, but this is not the norm. Sometimes the first round doesn’t help at all: this is completely normal, so don’t worry.
One study found optimal results took at least four visits, but some sub-types took more. With three months in between every round, you’re looking at a process that can take a year to dial-in the injections.
Why? Usually the doctors start with a lower dose than they think you need, and then slowly work up from there in subsequent appointments. The doctor will also probably start with obvious muscles to inject first, before slowly adding others or trying different muscles based on how you respond. This is done to avoid side effects and to evaluate what’s helping or not. In other words, botox injections for CD are not a simple paint-by-numbers task like other types of injections: it’s a process of trial-and-error.
Anecdotally, this is what we consistently see as well: it’s usually around the fourth round that people say they finally felt significant relief after a few rounds of trialing the injection locations and dosages with their doctor. Take good notes in between botox rounds and give your doctor clear and specific feedback so your doses and injection sites can be fine-tuned for your next round.
In other words, you need to have patience, but ideally each round will get incrementally better and better. The benefit from injections is a marathon, not a sprint.
Once you and your doctor have figured out the right muscles and the right dosages, your doctor will repeat the injections at regular intervals (usually every three months), but there may still be fine-tuning to be done in between rounds, especially if your dystonia changes, so continue to give your doctor feedback before every round. One study found CD patterns remained stable in 64% patients receiving injections, but 19% of patients saw their pattern become simpler involving fewer muscles, while 17% saw their pattern become more complex.
If it’s been a few rounds and you’re still not finding relief, it may be time to find a new doctor. Check out the question later in this FAQ, “What should I do if the injections aren’t helping me?“, for more detailed info on next steps.
7. How should I prepare for the injections?
You don’t need need to do anything specific to prepare for injections, but it’s not a bad idea to make sure you’re hydrated and you’ve eaten.
In the days before, you could consider taking zinc supplements. Some small studies (1, 2) suggest taking zinc for a few days before injections makes botox last longer. (Here is the full text of the second study.) (But another study could not replicate those findings.) It is a fact that botulinum toxin needs zinc in the body to work, so it makes sense to make sure you’re not deficient in zinc, which can especially be the case with vegetarians and vegans. Talk to your doctor before taking zinc supplements.
Unless you have a phobia of needles that causes you problems, you should be absolutely fine going to your appointment on your own without any assistance.
8. What sort of post-injection aftercare should I do?
After getting the injections, don’t put heat on the area for at least 24 hours as that can weaken the botox. Don’t put ice on or cool the area for an hour as that can reduce muscle uptake of the injection.
Don’t massage the area or do strenuous exercise within 24 hours because it can cause the toxin to move around beyond its intended muscle targets. Don’t lie down for at least four hours for the same reason.
One study suggests allowing the unwanted muscle movements within the first hour after injections helps the botox uptake into the targeted muscles.
Unless you have a phobia of needles that causes you problems, you should be absolutely fine going to your appointment without any assistance, including driving yourself to and from your appointment.
After the injections, take good notes in between botox rounds and give your doctor clear and specific feedback so your doses and injection sites can be fine-tuned for your next round. Ideally, you can visit your doctor for a follow-up after about six weeks so they can directly observe the effects of the botox.
9. How long do the shots take to work?
Everyone is a little different in how their body metabolizes the toxins, and different brands act a bit differently too.
If the injections worked, after about two weeks you should start to notice less pulling, less pain and/or less tremors. For some people or for some brands of injections, this can happen a little faster or slower than two weeks.
You may actually feel a bit worse in the first week until the effects start to kick in and your body adjusts – this is normal. You could feel some soreness as other muscles are compensating for having to work more.
Peak effect is expected somewhere between the two-week and six-week point.
However, if it’s your first round, you may not notice them ever really kicking in. That’s normal, so don’t worry. Why? Your doctor probably started you on a low dose to see how you respond – a typical starting dose for Botox and Xeomin is 100 units, but most people need more than that. Your doctor will raise the dosage incrementally. The doctor will also probably start with obvious muscles to inject first, before slowly adding others or trying different muscles based on how you respond. This is done to avoid side effects and to evaluate what’s helping or not.
In other words, you need to have patience as it can take a few rounds for you to really feel the shots helping, but ideally each round will get incrementally better and better. One study found optimal results took at least four visits (which takes one year), but some sub-types took more. Take good notes in between botox rounds and give your doctor clear and specific feedback so your doses and injection sites can be fine-tuned for your next round.
10. How long do the injections last?
Ideally, the injections will last 90 days until your next appointment for injections, but many people report the effects lasting less than that, i.e. 10 weeks. As the injection wears off, your symptoms will start to come back.
If they are wearing off too early, discuss with your doctor to see if a different toxin brand or a higher dosage would help. One study found higher doses (above 180 units of Botox) lasted longer than smaller ones (below 180 of Botox).
Some studies indicate that doing physical therapy in between botox injections can make them last longer (1, 2, 3). Ask your doctor how soon you can do PT. (You can read more about PT in our other FAQ here.)
Some small studies suggest taking zinc for a few days before injections makes botox last longer. (Here is the full text of the second study.) (But another study could not replicate those findings.) It is a fact that botulinum toxin needs zinc in the body to work, so it makes sense to make sure you’re not deficient in zinc, which can especially be the case with vegetarians and vegans. Ask your primary doctor before starting zinc.
Your doctor will repeat the injections at regular intervals (usually every 90 days), but you should continue giving feedback to your doctor before every round. Be specific about what symptoms have improved but which are still bothering you so your doctor can refine the injection strategy. One study found CD patterns remained stable in 64% patients receiving injections, but 19% of patients saw their pattern become simpler involving fewer muscles, while 17% saw their pattern become more complex, which means communication with your doctor is critical.
11. Are there side effects from the injections?
On the day of injections, usually there’s not side effects. Some people think the shots hurt, some people can’t feel them – the needle used is very thin, and it’s going into a muscle, not a vein or a nerve, so it shouldn’t be very painful.
In the following days, you might feel soreness and inflammation in the muscles that were injected. You might actually feel a little worse for a few days because the dystonic muscles get “angry” from the injections. This is normal.
Side effects in the following days aren’t super common, but the ones that occur most frequently tend to come from too high a dosage and the location where it was injected. In all cases, the side effects go away as the botox wears off:
- Trouble swallowing (more common when the lower part of the SCM is injected, or when both SCMs are injected – more info from a neurologist here)
- Head dropping/weakness (may be due to too much in semispinalis)
- Pain (if a nerve is hit, which is rare)
- Flu-like symptoms (aka “botox flu” – not very common)
One study following 235 various dystonia patients over 10 years of treatment cycles found side effects occurred in just 4.5% of treatment cycles, and 27% of people experienced a side effect at one time or another. In other words: Side effects aren’t that common.
If you have a disorder that causes hypermobility, like certain types of Ehlers Danlos, make sure your doctor knows before doing any botox as it can cause head instability in people with hypermobility. You may want to seek out a doctor who has experience treating CD in people with hypermobility.
12. Which muscles should I get injected?
Cervical dystonia is broken down into four sub-types based on the position the head wants to go in, and there are recommended muscles to be injected for each. But most people have a combination of sub-types, so it’ll be up to your doctor to figure out which are involved in your specific presentation – that is where EMG can help. The four sub-types are:
- Latero- head tilt, ear to shoulder
- Torti- head rotation or turn, chin to shoulder
- Retro- head pulling back, looking up
- Ante- head pushing forward, looking down
The so-called “col-cap concept” distinguishes movement that happens at the base of the head (“caput”) vs. movement that happens further down the neck (“collis”). Combining the four sub-types with the col-cap concept gives you eight distinct types:
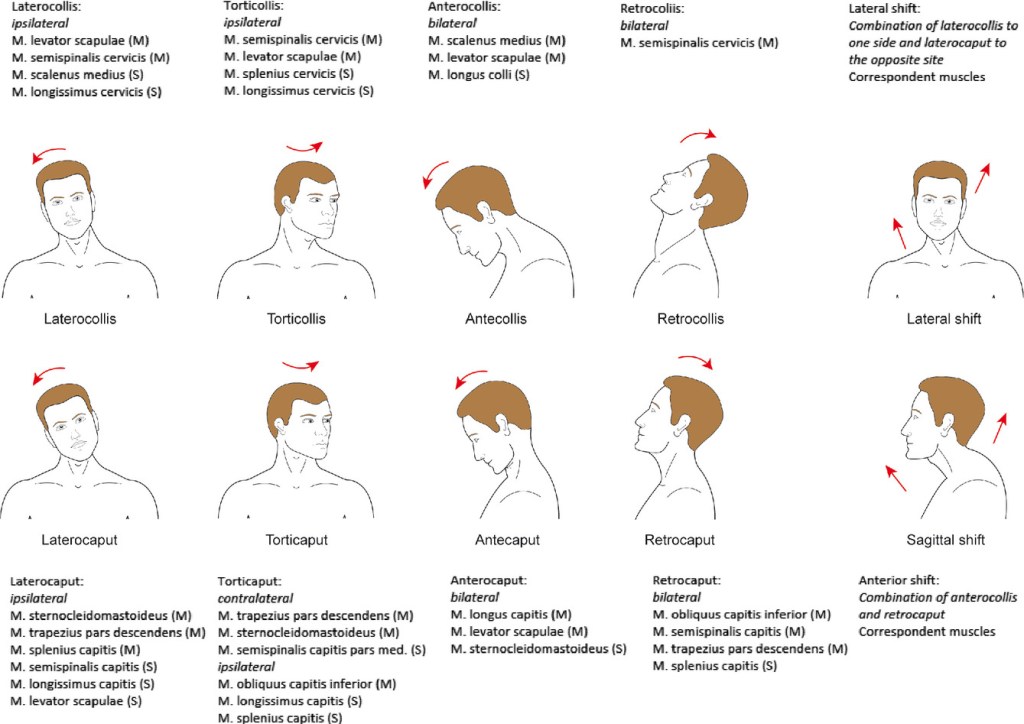
(Ipsilateral = muscles on the same side as the head turns or tilts toward. Contralateral = opposite of side of turn/tilt. Bilateral = muscles on both sides.)
This is not an exhaustive list as everyone is different, but some general guidance…
Laterocollis (all muscles on same side as lateral neck bending):
- Levator scapulae
- Semispinalis cervicis
- Scalenes (ultrasound recommended)
- Longissimus cervicis
- Longus colli
Laterocaput (all muscles same side as lateral head tilting):
- SCM/Sternocleidomastoid
- Upper trapezius
- Splenius capitis
- Semispinalis capitis
- Longissimus capitis
- Levator scapulae
Torticollis (muscles on same side of direction neck/head turns toward and faces):
- Semispinalis cervicis
- Levator scapulae
- Splenius cervicis
- Longissimus cervicis
- Scalenes (ultrasound recommended)
- Longus colli
Torticaput – muscles opposite side of direction head turns toward and faces:
- Upper trapezius
- SCM
- Semispinalis capitis
- Muscles on the side same:
- Obliquus Capitis Inferior/OCI (use ultrasound)
- Longissimus
- Splenius capitis
Retrocollis (muscles on both sides of neck bending up):
- Semispinalis Capitis
- Splenius capitis
- Semispinalis Cervicis
- Levator scapulae
Retrocaput (muscles both sides of head tilting up):
- Obliquus Capitis Inferior/OCI (use ultrasound)
- Semispinalis Capitis
- Trapezius (pars descendens)
- Splenius Capitis
- SCM
Anterocollis (muscles on both sides of neck bending down):
- Scalenus medius/posterior (ultrasound recommended)
- Levator scapulae
- Longus colli
- Sternocleidomastoids
- Scalenus anterior
Anterocaput (muscles on both sides of head tilting down):
- Longus capitis
- Levator scapulae
- SCM
Further reading on muscle selection for injections:
- https://www.nasafordoctors.co.za/articles.php?cid=4&id=6&aid=581
- https://www.nasafordoctors.co.za/articles.php?cid=4&id=6&aid=596
- https://movementdisorders.onlinelibrary.wiley.com/doi/10.1002/mdc3.12172
Studies show the most commonly injected muscles among all CD patients are:
- Splenius capitis
- SCM
- Trap
Here is a rough guide of how much botox is injected into each muscle on average. Usually, if you’re getting Botox or Xeomin, your doctor will start around 100 units and increase the dose from there in subsequent injections until the right dose is figured out. If you’re getting Dysport, your starting dose should be closer to 300 units.
Studies show multiple injection sites rather than one per muscle yields better results.
This 3D map of the neck muscles might be useful too: https://www.innerbody.com/anatomy/muscular/head-neck
13. Can botox reduce or eliminate tremors?
(Tremors are often associated with CD but not always. One study of 293 patients with CD at one medical facility found tremors present in 58%. Another study of 118 patients found tremors in 38%.)
Yes, botox injections can absolutely reduce or eliminate tremors – it’s just a matter of your doctor finding the right muscle with EMG.
There are generally two types of tremors: yes-yes (up-and-down, as if nodding “yes”), and no-no (side-to-side, as if shaking the head “no.”)
In yes-yes, usually you’ll need injections on both sides of your neck including the semispinalis capitis muscles and the SCM (sternocleidomastoid). You may also need the splenius capitis. Sometimes, you’ll need to add levator scapulae and/or the longissimus capitis.
For no-no, traditionally doctors will always inject the splenius capitis – your doctor will probably look at injecting one or both of your splenius capitis to address tremors. They may also inject the semispinalis capitis. However, one study found that the OCI (obliquus capitis inferior) is the most common muscle involved in no-no tremor. This study demonstrates how clearly ultrasound can visualize the OCI causing the tremor.
Here’s why the OCI is worth pointing out: The OCI is a deeper muscle best targeted with ultrasound to find and accurately inject. So, if you are not having success eliminating tremor with injections without ultrasound into muscles like your splenius capitis, you may need to try to find a provider who can use ultrasound to inject the OCI muscles.
See our explainer on which muscles you need injected for different types of CD in the previous question.
Some more info on injections for tremor: https://www.nasafordoctors.co.za/articles.php?cid=4&id=6&aid=586
14. Should I do physical therapy if I’m getting injections?
Yes! Studies (1, 2, 3) show that PT used in between botox injections is more effective than either PT or injections alone. You can read more about the different types of PT available in our other FAQ here.
Usually it’s recommend to wait a bit before doing any PT or massages on the area injected so the toxin stays where the doctor wants it.
15. What should I do if the injections aren’t helping me?
First: Have you given it enough time to work?
While injections do help most people, it often takes several rounds to figure out the correct combination of muscles and doses. CD is different in everyone, and there is usually trial-and-error involved. Your doctor wants to weaken the dystonic muscles enough to stop the pulling, but not so much that you have other side effects. So, they usually start at a lower dose and fewer muscles than they think you need and work up, so it can take a few rounds to get right.
There are more than 20 different muscles in the neck that your doctor may need to inject – think about how many possible combinations are out there, and your doctor needs to find the perfect one for you. Make sure you give your doctor clear and detailed feedback after and before every round. If you’re not satisfied with your results, say so, and say what symptoms you still feel and exactly where so your doctor can refine his/her approach.
One study found optimal results took at least four visits, but some sub-types took more. With three months in between every round, you’re looking at a process that can take a year. Another study found efficacy of the injections improved each visit for 13 visits (more than three years) before holding steady. One study found patient satisfaction with the injections increased after 5 years.
So, the first thing you need to do is be patient and give it three or four rounds. Do not give up after just a couple rounds!
But what if you’ve given it several chances to work and it still hasn’t?
Second: Have you tried switching doctors?
When injections don’t work after a few tries, some people assume they are immune or botox won’t work for them. This is usually not the case as the incidence of immunity is low, especially in someone who has only had a few treatments. Studies show poor results are usually because whoever is doing the injections is doing it wrong, so, this takes up the next step: the best thing to do if you’re not satisfied is consult with a new doctor and try again.
If your doctor is not using EMG or is not a movement disorder specialist (as discussed earlier in this FAQ), then it’s especially recommended to switch doctors immediately. But even an experienced movement disorder specialist may not be the right fit for you.
In one study of people who got poor results or no results, 78% of patients had better outcomes after being re-evaluated by different doctors and re-trying injections. The most common reasons cited for the bad results was (1) wrong dosage (2) wrong muscles. The study authors concluded: “These results indicate that the majority of unsatisfactory responses to BoNT treatment of CD were caused by correctible factors and imply a need for improved education regarding optimal treatment methods.”
A different study of people with sub-optimal botox results was similar, and most of the patients (60%) got better results when the dosage, muscle selection or injection technique was changed.
This matches with what we see anecdotally a lot: people have bad results but switch doctors and start getting good results. The opposite can also happen, unfortunately: someone has good results, but they move or their doctor retires, and their next doctor doesn’t get the same good results. See the next question in this FAQ for more.
Some forms of CD are trickier than others, too. The torti- (head turn) and latero- (head tilt) forms are more common and usually require injecting superficial muscles. Anterocollis and anterocaput (head looking down) are considered the most complicated forms to treat because the muscles that have to be injected are deeper in the neck. Finding an experienced doctor in antero- forms and/or who uses ultrasound might lead to better outcomes. (Further reading on antero- forms here.) No-no tremors can also be trickier than yes-yes tremors – see question #13 of this FAQ for more info on treating tremors with botox.
Third: Have you tried switching toxins?
What if you’re still not getting results? Trying a different toxin can also help sometimes. Anecdotally, some people say Botox never helped them, but as soon as their doctor switched to Xeomin or Dysport, they started getting great results. And vice versa. Although the toxins are all very similar, everyone is different.
If you did develop resistance to Botox or Dysport (again, it’s rare), switching to Xeomin usually works – the formulations are different and Xeomin is more “pure” without accessory proteins, so your body probably won’t recognize it if it developed immunity to Botox or Dysport. If none of the type-A toxins work (Botox, Xeomin, Dysport or Daxxify), then you can switch to type-B (Myobloc) and it should work because it’s a different active ingredient.
Bottom line: Please give botox a few rounds before giving up, and please switch doctors if you haven’t gotten results after multiple rounds. Let the new doctor re-evaluate you and try their own fresh approach with injections.
That said, botox is not a 100% guarantee. Some people don’t respond well enough after giving it many attempts, so they rely on medications and other treatments, or are referred for a surgical option, which is explained in the other FAQ.
One other less likely possibility worth mentioning: If you have “functional dystonia” rather than true, organic dystonia, botox probably will not help you, so having the correct diagnosis is very important. Functional dystonia is a type of functional neurological disorder, or FND. It’s explained in the last two questions of this FAQ here.
16. Is it really worth it to try switching doctors if botox hasn’t worked? Why would that help?
Both the research and tons of anecdotal experiences are clear: If botox injections aren’t helping, the best thing you can do is switch doctors and try again. This is true even if you have already been seeing a movement disorder specialist who has experience with CD.
A different doctor may be better at identifying your dystonic pattern, which means injecting different muscles or changing how much botox you get in each muscle. Every case of cervical dystonia is unique and there is no cookie-cutter approach that applies to everyone. There are more than 20 different muscles in the neck that your doctor may need to inject, and despite the many possible combinations, your doctor needs to find the perfect one for you.(See question No. 12, “Which muscles should I get injected?” for more explanation on the complexity of identifying the correct muscles for each pattern.)
Again: In one study people who got poor response and no response to injections, 78% had better outcomes after being re-evaluated by different doctors and re-trying injections. The most common reasons cited for previously having poor results was (1) wrong dosage (2) wrong muscles.
But what if you already know which muscles you need injected, or maybe you’re already at the max dose? You may be wondering: Why would different doctors get different results if they are injecting the same muscles?
Well, it may come down to your anatomy and the doctor’s injection technique. Studies show that botulinum toxin works best when injected closest to a part of the muscle called the motor endplate, which generally lies in the center of the belly of the muscle within the neuromuscular junction. If your doctor isn’t injecting deep enough, or is injecting too deep, they might just be missing it.
For example: the average thickness of the sternocleidomastoid, or SCM (one of the most commonly injected muscles in CD), is only 5 millimeters, per research. That’s about the length of a grain of rice or the eraser on top of a pencil. As you can see, there’s not much margin to work with to hit the exact needed location. Someone with CD may have a thicker SCM than normal, but that only means it may be even harder to find the center belly of the muscle and it would be easy to not inject deep enough. (This is another reason why finding a doctor who also uses ultrasound, in addition to EMG, may be beneficial.)
Again, we know both anecdotally and from research that if you aren’t getting results from botox after a few rounds, the best thing you can do is try another doctor. Remember that one study where 78% of patients had better outcomes after being re-evaluated by different doctors, and the most common reasons cited for poor results were (1) wrong dosage (2) wrong muscles? Well, reason (3) was listed “undetermined” meaning switching doctors just helped for a reason that wasn’t obvious. Another study of people with sub-optimal responses was similar, and most of the patients (60%) got better results when the dosage, muscle selection or injection technique was changed.
This matches with what we see anecdotally in support groups a lot: people have bad results and switch doctors, and start getting good results. Some people find that when they switch to a doctor and start getting better results, that doctor doesn’t need to use as much botox either.
Botox injections for CD require more finesse and nuance than other types of injections you might be used to – that’s why the experience, skill and willingness of the injector is so important. It is not a simple “paint by numbers” task.
17. What should I do if the injections stopped working?
When you used to get a good response but injections have stopped being effective, this is called “secondary non-response.”
First, consider if your treatment has changed. Did you switch doctors? We see it all the time: people have bad results and switch doctors, and start getting good results. The opposite can also happen, unfortunately: someone has good results, but they move or their doctor retires, and their next doctor doesn’t get the same results. If you’ve switched doctors and your injections aren’t helping like before, your new doctor may not be a good fit. That’s true even if your new doctor is doing the exact same injections as your previous doctor – see the previous question for further explanation.
Second, you should determine if your CD has changed. Many people find their dose needs to increase over the years, and studies find secondary non-response is often due to CD getting worse. Sometimes, the pattern of dystonic muscles can change in response to botox injections because the CD is caused by the brain trying to hold the head in certain positions rather than activating specific muscles.
The odds of developing resistance to botulinum toxin injections is quite low and it’s relatively rare. Even so, if you did develop an immune response, it usually helps to switch brands of toxins. Xeomin is a more pure form, so switching to that brand from Botox can help. If neither of those work, there is a formulation that is different than all the others called Myobloc.
If that still doesn’t help, often the next step is a surgical option, which is explained in our other FAQ.
18. I heard botox only helps a small percentage of CD patients – is that true?
No, it’s not true. Multiple studies show most people who get botox injections see improvement. (Here are a few studies with the percentage of people benefitting from injections: 80%, 85%, 86%, 64%, 85%.)
I’m not sure why you see some people with CD claiming on social media that botox only helps a small percentage of CD patients – it’s not only inaccurate, it’s harmful because it encourages people to give up on the treatment before it has the chance to help. Remember: As we covered earlier in the FAQ, studies show it takes about four rounds for botox to work well, which is process that can take a full year. Don’t give up before it has the chance to help.
If botox isn’t helping you, the best thing you can do is switch doctors, get re-evaluated and try again. Make sure your new doctor has experience with CD and uses EMG guidance. In one study of poor-responders and no-responders, 78% had better outcomes after being re-evaluated by different doctors and re-trying injections. The most common reasons cited for poor results were (1) wrong dosage (2) wrong muscles. Another similar study found most patients (60%) got better results when the dosage, muscle selection or injection technique was changed. (See more explanation in question #16.)
I would add: the people having poor results from botox are going to be far more visible in support groups. People will post (1) when they are just starting botox and haven’t gotten it dialed in, or (2) when they are unhappy with their botox results. But rarely do people post to share they got great results, or to share that they are consistently getting great results every three months.
19. Can I get injections more often than every 3 months?
Maybe, but you probably shouldn’t, for two reasons:
- A small percentage of people can develop an immune response to the injections, which causes them to stop working. The odds of your body producing antibodies to block the toxin increases a) the more frequently you are injected, b) the higher the doses you get, c) the longer you’ve been getting the injections. By waiting three months, you’ll keep your odds low.
- If you’re in the U.S., your insurance company probably will not pay for injections more often than every 90 days, which is almost 13 weeks. You should check your insurance coverage documents to be sure, but usually you are limited to injections once every 90 days and no sooner. Some insurance plans may allow a more frequent basis if requested by your doctor and with evidence 90 days isn’t frequent enough, but they will likely need to pre-approve that.
Some people who don’t have to deal with the American health insurance system do get their injections more frequently than every 13 weeks (i.e. every 11 weeks) but the general consensus is you should not get injections any sooner than every 10 weeks.
Some small studies suggest taking zinc for a few days before injections makes botox last longer. (Here is the full text of the second study.) (But another study could not replicate those findings.) It is a fact that botulinum toxin needs zinc in the body to work, so it makes sense to make sure you’re not deficient in zinc, which can especially be the case with vegetarians and vegans. Ask your primary doctor before starting zinc.
There is a newer formulation called Daxxify that is supposed to last longer than Botox, Xeomin and Dysport. See the next question.
20. What are the differences between the various botulinum toxin brands?
Although people colloquially refer to these injections as “botox injections” — and we do too in this FAQ, with a lowercase B — there are multiple brands available.
Botox (onabotulinumtoxinA): This is the oldest and most well-known, and the pioneer of using botulinum toxin to treat dystonia. After years of research, in 2000 it was approved in the U.S. as treatment for CD (two years before it was approved for cosmetic uses!), and it has been a treatment of choice ever since. (Here’s a history of Botox being discovered as a treatment for CD.)
Xeomin (incobotulinumtoxinA): This is a purer form that lacks added proteins compared to Botox. As a result, it seems to be slightly less likely to produce an immune response. If people stop responding to Botox, switching to Xeomin often gets a response again. It may be cheaper than Botox too because it doesn’t need to be stored at a refrigerated temperature like Botox. Same ratio as Botox, so one unit of Botox is equal to one unit of Xeomin. It was approved by the FDA for cervical dystonia in 2010.
Dysport (abobotulinumtoxinA): Approved by the FDA in 2009 for CD treatment. Its manufacturing process is a little different than Botox and Xeomin. It appears to spread in the muscles more easily than the others, which can help when trying to treat larger areas, but can potentially lead to more side effects when it spreads beyond the intended target. Its dosing is different, a 3:1 ratio with Botox and Xeomin.
Daxxify (daxibotulinumtoxinA): This is the newest one, having only been approved by the FDA for CD treatment in 2023. It claims to last longer than the others – around four or five months instead of three. As with all these injections, individual patient experiences vary. Like Xeomin, this doesn’t contain added proteins. Daxxify dosing is around 2:1 (maybe closer to 1.5x) compared to Botox. Anecdotally, some people who get Daxxify say it stings a little more during injection.
MyoBloc (rimabotulinumtoxinB): While all the others are type-A toxins, this is the only type-B available. This formulation doesn’t work as well as type-A, but in people who have built resistance to type-A or don’t respond to type-A, this is an alternative that can work. This one has been used for CD since 2000 in the United States. Dosing is different and much higher than the other forms.
Which one should you choose? You’ll want to discuss that with your doctor. Studies show Botox, Xeomin and Dysport last a similar amount of time. Daxxify is the outlier that is supposed to last much longer than the rest, but everyone’s individual experience is different, and some people do not have longer results with Daxxify. In terms of how well they work, all the type-A formulations are similar and results vary person to person. Anecdotally, sometimes people say different brands worked better for them (i.e. Botox didn’t help them, but Dysport did; or Xeomin didn’t help them, Botox did) but chemically all of the toxins are very similar.
[There is an ongoing trial for a new type of toxin that will (hopefully) last up to six months. More details are here. You can probably volunteer to try it yourself!]
21. Are there long-term concerns about getting botox injections?
No, there don’t appear to be long-term side effects or concerns based on all available evidence.
This review looked at various studies, including one that followed various dystonia patients (including CD patients) for 16 years and found no significant changes in how well the injections worked and patients actually seemed to experience less side effects compared to early on in treatment. Other studies cited in this review looked at patients over 10-year periods, and similarly found the shots remained effective and the incidence of side effects was low.
This study looked at patients getting botox injections for at least 15 years and as long as 26 years for CD and other conditions. Again, the study found persistent benefits with minimal side effects.
Anecdotally we’ve met people who have gotten Botox injections for 25 years (since as long as it’s been approved by the FDA for cervical dystonia) without issue and say it has allowed them to live completely normal lives: worked full-time jobs, got married, had children, etc.
A recent study in Wales looked at all CD patients in the country over the course of 23 years and found life expectancy was the same as the general population.
After botox wears off, muscle function and strength are generally restored to normal levels very quickly. One very small study of cervical patients found strength in neck muscles returned to baseline within 12 weeks after injection.
A very small study of hand dystonia patients found minor muscle weakness in some people after the injection would’ve worn off, as long as 3.5 years after the last injections. (Arguably, this is good and would demonstrate botox could potentially help people with dystonia longer than 3 months – but the reduced strength found in the study of 11%-13% is quite minor.) The study concluded that “the observed long-term side effects of BoNT remain subtle, emphasizing its safety over longer periods of time.”
22. How do I pay for injections?
Even with commercial insurance, the injections can result in some pretty hefty bills if you live in the United States. (Even after meeting my deductible, I pay 20% per session, which is around $600.)
Thankfully, all the toxin manufacturers offer discount programs that can bring your net out-of-pocket cost to $0 if you have commercial insurance. These savings programs cover the cost of the toxin itself AND the doctor’s charge for performing the injections, up to around $1000 per treatment after what your insurance pays.
For those without insurance who meet income limits, companies have assistance programs to help pay for injections.
- Botox (with insurance): https://www.botoxsavingsprogram.com/
- Botox (assistance): https://www.abbvie.com/patients/patient-support/patient-assistance.html
- Xeomin (with insurance): https://merzconnect.com/patient-xeomin/patient-savings
- Xeomin (assistance): https://merzconnect.com/patient-xeomin/patient-assistance-program
- Dysport (with insurance): https://www.ipsencares.com/dysport-patient-support
- Daxxify (insurance+assistance): https://hcp.daxxifycervicaldystonia.com/access-daxxify
- Myobloc (insurance+assistance): https://www.myobloc.com/financial-assistance-faqs-resources
A note that U.S. health insurance companies usually want prior authorization for injections, and if anything changes about your treatment, they may ask for a new prior authorization request.
So, if your doctor wants to go from 100 units of Botox to 200, that may require a new prior authorization request. If you switch doctors, again that may require a new prior authorization request, and may require the old doctor’s authorization request to be formally withdrawn.
It can be a hassle, but to avoid delays in treatments, it’s worth staying on top of your insurance company and your provider to make sure everything is being done right if anything changes about your care. Also, prior authorization requests are often valid for only one year, so a new one needs to be submitted to your insurance annually.
Last updated:
